





Integrated healthcare systems: Benefits and structure

June 10, 2026 10 min read 55 views
The healthcare industry is rarely simple. When treated by a primary care provider (PCP), individuals often see multiple PCPs before returning to their original PCP for follow-up. How do we know all the different providers involved in our patient’s care are connected?
Integrated health systems are intended to connect multiple providers to facilitate tight integration among service delivery, provider teams, and patient health records. By doing this, patients can have timely access to their providers and receive appropriate referrals, enabled by the timely transmission of health records.
Providers benefit from integration by improving communication and gaining a better understanding of the patient’s needs. As a result, the quality of care provided to patients will improve throughout the healthcare system over time.
Integrated healthcare model key takeaways
- Integrated healthcare connects providers, systems, and services to reduce fragmentation across the patient journey.
- Vertical, horizontal, and virtual models support integration in different ways, depending on structure and goals.
- Clinical and administrative integration both matter: one improves care delivery, the other supports its operation.
- Interoperability, shared standards, and realistic implementation planning are essential for making integration work in practice.
What is integrated healthcare?
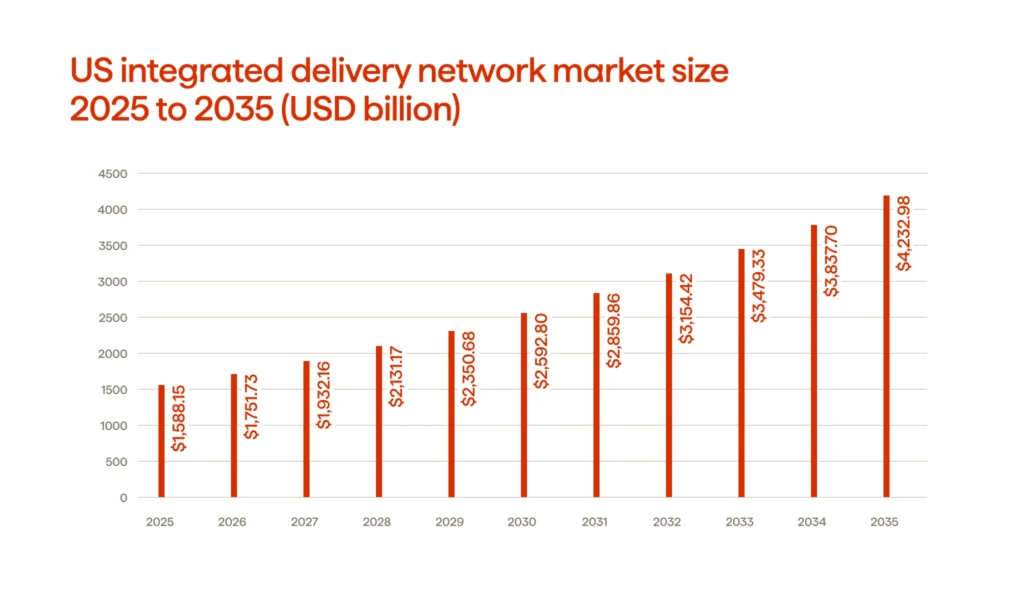
A report published by Nova One Advisor reveals that the Integrated Delivery Network (IDN) industry in the United States will be worth $1,588.15 billion by 2025 and is projected to reach $4,233 billion by 2035. This represents a significant shift in attitudes about integrated delivery networks. By viewing integrated delivery networks as a primary focus within the healthcare field (rather than just as a peripheral initiative), healthcare providers now view these networks as an integral part of their overall business strategy.
A model of integrated healthcare involves bringing together various healthcare professionals into a cohesive system. When health care services are fragmented, these types of activities become disassociated from one another, creating delays in communication and decision-making.
The goal of integrated health care is to improve care management across a multidisciplinary team by having all team members share a common electronic health record. The result? A single, shared view of each patient’s clinical information.
Defining healthcare integration: vertical, horizontal, and virtual models
Usually, three forms of healthcare integration occur: vertical, horizontal, and virtual. Each type links services differently but is designed to create a more seamless patient experience and reduce fragmentation in care delivery.
Vertical integration involves connecting multiple services at all levels. For example, a hospital system could partner with its affiliated community-based primary health care clinics to provide continuity of care to patients from diagnosis through treatment to recovery, while also sharing information and coordinating decisions among providers at different levels of care (e.g., hospitals vs. outpatient clinics).
Horizontal integration occurs among providers that provide similar service types at the same level of service. For example, a hospital could join forces with another hospital to form a larger network of facilities, or a group of primary care clinics could work together to operate under one umbrella organization. This type of integration is commonly used to standardize service delivery processes, expand access to care, and reduce redundancies. Additionally, horizontal integration helps organizations manage their resources more effectively across multiple locations.
There is greater flexibility with virtual integration. Two or more organizations can remain separate entities while coordinating and collaborating through common protocols, referral pathways, data sharing, and various forms of digital technology. This type of virtual integration is becoming increasingly prevalent in integrated care today, as many organizations seek to coordinate within their systems without taking on complete ownership or merging. Additionally, virtual integration can be beneficial for developing a comprehensive health care model that incorporates all aspects of medical, behavioral, community, and social support services.
No single system will work for every organization; some organizations use a single framework, while others use multiple ones. Ultimately, what counts is whether the combination of all three types of systems will strengthen collaboration among physicians and other health professionals when collaborating as a team to provide better patient care.
| Model | How it is structured | Main focus | Typical participants | Best fit |
|---|---|---|---|---|
| Vertical | Links different levels of care | Continuity across the patient journey | Hospitals, specialists, rehab, long-term care, primary healthcare | Managing care across multiple care settings |
| Horizontal | Combines services at the same level | Scale, consistency, shared operations | Hospital groups, clinic networks, labs | Expanding reach and standardizing delivery |
| Virtual | Independent providers coordinate without a full merger | Flexibility and collaboration | Clinics, hospitals, community services, digital partners | Coordinated care systems with less structural change |
Clinical integration vs. administrative integration
The differences between administrative integration and clinical integration are straightforward: clinical integration concerns how care is delivered, while administrative integration concerns the behind-the-scenes processes that support that care.
Clinical integration examines how patients experience receiving care and how they receive coordinated treatments. Clinical integration ensures that patients do not receive disconnected services when treated by multiple professionals by developing teams of providers, including a primary care physician, specialists, nurses (including physician assistants), and a care coordinator. This is particularly helpful for those with multiple conditions or who will require long-term support.
As an example of how clinical integration works, combining behavioral health and primary health care along a single set of pathways integrates patients’ mental and physical health into a single service. One of the primary goals of clinical integration is to ensure continuity of care; support better decisions and outcomes for individuals through improved communication and coordination; and help improve long-term health by hardwiring clinical integration principles into day-to-day business practices.
Administrative integration involves coordinating budgets, scheduling, human resource functions, information technology, compliance activities, procurement, and reporting across the entire Delivery Network. This work is done behind the scenes and is often not visible to the patient. However, patients will experience an indirect impact. When administrative functions are not integrated, it takes longer to make referrals, records are less easily accessible, and service access is less reliable. By integrating administrative systems, organizations can better support their care teams and achieve consistent operations across all locations.
| Aspect | Clinical integration | Administrative integration |
|---|---|---|
| Main focus | Coordinated patient care | Coordinated operations and management |
| Who is involved | Doctors, nurses, health workers, therapists, care coordinators, and primary care teams | Operations leaders, HR, finance, IT, compliance, and scheduling staff |
| What it improves | Treatment alignment, patient follow-up, integrated behavioral health, support for complex health conditions | Workflows, staffing, reporting, resource use, and access to services |
| Patient impact | More connected medical services and better long-term health support | Fewer delays and a more stable delivery system |
| Example | Shared care plans across primary care and behavioral health | Unified EHR, billing, scheduling, and referral processes |
Interoperability requirements and standards (FHIR, HL7)
In conventional health care systems, patient information can become locked into silos within different computing environments. For example, one clinic may record lab results differently from another; one hospital may document visits differently from another; and so on. This situation leads to high administrative overhead in integrated healthcare, as seamless data transfer is essential for every service a patient uses.
HL7 and FHIR are part of this process and are two of three different types of standards that include data exchange, integration, sharing, and retrieval of electronic health information. HL7 is the larger standards organization for creating standards surrounding electronic health record (EHR) data exchange, while FHIR is one of those newer standards for EHR data exchange (FHIR is an abbreviation of Fast Healthcare Interoperability Resources). FHIR was created with a focus on enhancing ease of implementation and enhancing the usability of web technologies in EHRs, making it a preferred integration standard for most current integration projects.
Interoperability is about how clinical data can be understood and used by all data providers, the systems they operate with, and the types of care services they deliver. An example would be that the client should receive an appointment update in a structured format that allows easy access and is not just for future reference. This type of interoperability will reduce redundant work and support a fast, coordinated team effort to provide better health care. The cost savings from reducing duplicative activities and delays, and eliminating unnecessary administrative costs, can also help control costs for the health care system over time.
So, if integrated care is the goal, interoperability is the infrastructure underneath it. Without shared standards, the connection stays partial. With them, care coordination becomes easier across the full patient journey.
Modernize CRM operations, enable omnichannel marketing, improve data utilization and sharing, accelerate regulatory content approval, and achieve greater customer engagement.
Common implementation pitfalls
Even carefully thought-out integration initiatives can encounter difficulties. In many instances, the problem lies not in the concept of an integrated healthcare system per se, but rather in how it is implemented, managed, and encouraged throughout the entire enterprise.
- Focusing on integration alone as a technology project. In many organizations, there is an emphasis on using platforms to facilitate data exchange while de-emphasizing workflows, roles, and accountability. To effectively integrate health care, organizations also need to create operational changes (not just provide new tools).
- Maintaining siloed decision-making between departments. By continuing to operate according to their own departmental priorities, integration will never be complete. Shared governance is essential for teams to carry out their goals toward healthy populations.
- Frontline clinicians are not adopting new systems. New systems may look perfectly functional on paper; however, they can fail if not properly trained during implementation or if there is no immediate application for the new tools.
- Data of poor quality and low interoperability hampers the coordination of high-quality healthcare delivery across multiple settings when data is incomplete, inaccurate, or inaccessible.
- Unresolved care coordination. Patients with complex needs frequently move from one team to another. Due to a lack of an established primary provider, follow-up care may be delayed, duplicated, or completely missed.
- Attempting to recreate current systems and processes into a new model. Some organizations are simply digitizing current processes without determining whether those processes still make sense in a more integrated environment.
- Underestimating the level of change fatigue in staff. Staff may already be experiencing change fatigue due to ongoing multiple system updates, compliance requirements, and staffing requirements. Many organizations that do not take this into account will lose momentum on integration efforts.
- Measuring activities as opposed to outcomes. More referrals, shared records, or meetings do not translate into better care. The real question is whether integrated care methods produce better outcomes than traditional care methods, as measured against baseline data points.
Clear ownership, usable systems, realistic rollout strategies, and shared priorities are typically the cornerstones of a successful integration architecture. Even a well-funded project may find it difficult to bring about significant change without them.
FAQ
Integrated healthcare approach: Wrapping up
Integrated health care will improve continuity for all patients rather than standardizing all of the services they receive. The more integration among the provider, system of care, and patient data, the fewer patient gaps will exist, leading to better decisions by care teams. This will impact your individual care as well as the overall way you will receive care. Integration is ultimately about the experience of receiving health care rather than the structure of the health system in writing. If care feels seamless, easily accessible, and easy to navigate, then integration has been successful.
Want to learn more about the benefits of integrated healthcare? Contact Avenga, your integrated health care system partner.


How supply chain visibility affects business operations

GIS for telecommunications: Enterprise network management
Your business results matter
Achieve them with minimized risk through our bespoke innovation capabilities. Fill in the form below.